February 23 – March 1: 36 Weeks 0 Days – 36 Weeks 6 Days.
The third trimester is supposed to be slow, or at least the last month of it. For me, time is passing faster than ever. Upon writing this, I can’t believe I’m already in my creeping up on my 38th week! (Or that I’m so behind of writing this blog post)
As work has wound down, I’ve begun to do more exercise and yoga for myself, which has been fantastic. I’ve been doing prenatal pilates once or twice a week since the beginning of my second trimester, and when I started seeing the chiropractor I began a daily gentle exercise routine that I do as part of my bedtime wind down. Now I’ve added on a prenatal yoga class (or two) a week, and an early-morning swim on the weekend. When I’m in my bikini (I didn’t bother to buy a pricey one-piece maternity swimsuit), it’s obvious that I’m pregnant; my navel is partially inverted and my belly’s skin is taut and shiny like one those rubber balls Walmart sells. It’s inevitable that I end up having a half-clothed conversation in the women’s locker room about pregnancy or birth, which is welcome and sweet—except for the woman who exclaimed, “It’s going to be twins!”
-

- Yoga Back at 30 Weeks. I missed my belly photo this week!

-

- Taken at Thriveability Yoga, which has an amazing prenatal yoga program.

-

- Photo Credit: Rachel Augustine

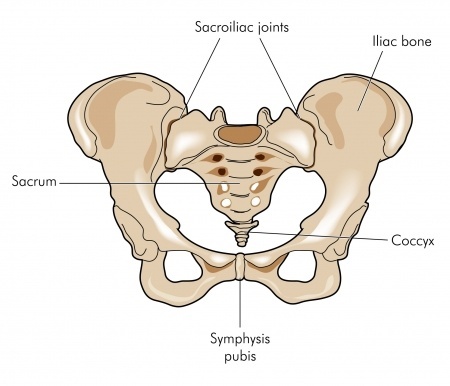
Even though my legs and arms are getting a little scrawny, I feel more aligned and fitter than I have at any other point in my pregnancy. Fit doesn’t mean what it used to though. I may feel especially healthy because I’ve come into acceptance of my limitations. For every minute of exercise I do, I need an equally long nap (or longer). And household chores count as exercise—I can only handle about one big chore a day, especially ones that involve bending over and lifting. The baby shifts up and down, but sometimes her head feels like it’s right against my cervix, which make my lower belly feel incredibly heavy and my pelvic joints ache. When walking, I have to take small slow steps or I get a shooting spasm down my inner thigh. This happens sometimes when the baby moves, too, so she’s probably compressing a nerve.
Now that I’m working less and less, I have time to accommodate for these discomforts, so it’s not so bad. And, what’s going on doesn’t feel unhealthy: it’s amazing that the baby is exploring her exit route, and I’ve been trying to avoid sending her negative signals. In her yoga classes, Britt Fohrman sometimes has us exhale with a joyful, sensuous “Mmmm…” sound, as if we’ve just had a delectable bite of our favorite sumptuous dessert (a birth technique). When the baby causes me discomfort, I try to respond with this technique instead of tensing up and groaning. However, with the shooting inner thigh spasm, it usually comes out as, “ArrrgmmMmmm…”
I’m hoping that staying active and practicing birth techniques when I get aches and pains now will set me up for a smooth labor. I used to visualize myself having a quick labor. I know I’m going to regret saying this, but with all the prep Richard and I have done now, it would be a little disappointing to have a superfast labor with no time to use the techniques we’ve learned. Also, I’ve heard a few birth stories from women who have had fast, intense labors, and apparently it’s mind-boggling to have earlylabor-activelabor-pushing-baby in a matter of hours—there’s no time to come into full acceptance of what’s happening. Now I visualize myself having a smooth, average-length labor, in which there’s time to experience each phase.
Contrary to most of the crisis-situation portrayals of labor in TV and movies, things usually start slowly with mild surges (contractions) that gradually get closer together, longer, and more intense (although there are always exceptions!). Most women don’t have to rush to the hospital upon their first contraction. I plan to labor at home for as long as possible (which is also the hospital’s preference. They’ll send me home if I show up too early).
All sources that I’ve read or heard tell women to sleep as much as possible early on while labor surges are still mild and spaced out. There are different opinions on what to do if I can’t sleep. My doulas and childbirth prep class teacher (both hypnobirthing-focused) say I should start practicing my birth techniques early. Natural Hospital Birth, a book I read several months ago, says that using coping strategies too early may burn me out on them, and by the time I really need them, they wont be effective any more. The author recommends coming up with a list of early labor activities to distract myself while the surges aren’t dominating my attention. I think it would be nice to do something in between: choose some gentle activities to do in between surges, and pause to practice my breathing and relaxation techniques during surges. I tried to come up with activities focus more on connecting me to my experience than distracting myself from it, and on getting me out of my analytic mind and into my intuition. Here are some of my favorite ideas on my Early Labor Activities list:
- Art therapy. A couple months ago I tried a wonderful art therapy technique. I drew an outline of my body, took some time to breath and meditate on the sensations I was experiencing (which I could do during a surge), then paint the sensations over the outline with watercolor paints. If I have any desire to sit upright, I think this would be lovely during early labor and leave me with a nice memento.
- Bake and decorate “welcome” cupcakes for the baby. Throughout pregnancy, I’ve made cakes and cupcakes for several big events (including the baby shower), and so it feels like a rite of celebration for me. I’m not convinced that I’ll actually have the energy to be on my feet baking (maybe Richard can help me out with that part), but I know decorating cupcakes with phrases like, “welcome” and “we love you” would help shift my perspective from pregnancy to motherhood. If I actually finish them, they would be a great treat to bring to the nurses’ station at the hospital too.
- Yummy exercises. I can see myself stretching my shoulders, rolling out my thighs and back on my foam roller, and easing jaw and neck tension with some pinky balls. This will feel good in the moment and get me limber and loose for labor.
- Have Richard read some pre-selected passages to me. Even though I’m not supposed to use the word “pain” with regard to my surges, I would love for Richard to read me a couple anecdotes about pain that I use when teaching yoga and meditation to patients with incurable chronic pain (some of whom feel the intensity of labor on a daily basis). I love the mantra, “Pain, the door of my heart is open to you,” as a reminder to soften to sensation rather than harden to it. However for the sake of positive language, I may adapt it to, “Intensity, the door of my heart is open to you.”
- Sing. Not sure if I should bother making a sing-along playlist now, or if whatever I choose in advance will just annoy me because I’ll be in such a different state.
Eventually I’ll end up the hospital, and this week I finally sat down with a Birth Preferences template my doulas provided, and modified it match my wishes. Since it includes so much from their template, I won’t post the full plan here, but here are some of the things that are important to me:
- If everything is going well, I want to be internally-focused and following my intuition without interruption and intervention. To support this, on my birth preferences I requested keeping hospital staff entering to a minimum, having them direct communication to Richard or my doulas if possible, using electronic fetal monitoring only as much as is necessary, and reserving cervical exams for when they inform medical decisions (rather than getting routine hourly exams just to see how dilated I am).
- I am well-educated about my options, and I’ve chosen my preferences based on what I think will yield the best outcomes for both the baby and me. Sticking to my preferences may not be easy, and I want my birth team to be supportive. One of my preferences is that my providers not offer me pain medication. If I want something, I’ll ask for it.
- Unless medically necessary (e.g. I get an epidural and can’t feel anything), I don’t want to be coached to push. Although coached pushing is typical in hospitals, there is evidence that it can cause the baby to come out violently (causing tears and other problems in the mother) rather than smoothly. Also, the uterus can push the baby a big chunk of the way out on its own once the cervix is fully dilated, so starting active pushing as soon as the woman is fully dilated can be needlessly fatiguing. (There’s a nice article about all this on BabyCenter if you want to know more). I trust that when it’s time to push my body will let me know. Update: A doula friend informed me that some women never get the urge to push. If I have a long, exhausting labor, I’ll keep an open mind around coached pushing.
- Saint Luke’s does delayed cord clamping by default (there’s evidence that this helps establish the baby’s iron stores), but there are different ideas about what “delayed” means. On my birth preferences I specifically ask for five minutes to ensure the cord has time to finish pulsating.
- I want the baby to experience the world as a safe, secure place she can trust, so I’ve requested that all newborn procedures be delayed until an hour and a half after birth. Hopefully we’ll get some quality skin-on-skin time and try out breastfeeding before the baby needs to be poked, prodded, and weighed.
I’ve had a few people tell me birth preferences aren’t worth writing down because you can’t predict what’s going to happen during labor. For me, I don’t see the harm. Worst case scenario: my labor is rife with medical emergency after medical emergency and no part of my ideal birth is achieved. Many of the points on my birth preferences are qualified with the equivalent “unless doing otherwise is medically necessary,” so even this would not really violate my birth preferences. Average case scenario: Some of my birth preferences can’t be met, or I change my mind about some of my birth preferences in the moment. My birth preferences are not a covenant with God. Nobody is going to tell me I can’t do something because it violates a list I wrote ahead of time. Best case scenario: My baby and I have an amazing, wonderful birth experience with care above and beyond what the hospital would normally offer (or more tailored to my personal ideal, anyway). I’m not willing to give up the possibility for the best case scenario for fear of feeling disappointment in the other scenarios.
All in all, I’m feeling confident and at ease about going into labor, with a hint of something that could be either nervousness or excitement. You can come whenever you’re ready, little one!